Vaginitis and PID Wanda Ronner, M.D.. Vaginitis Disruption in the
$ 9.00 · 4.9 (371) · In stock
Normal physiologic discharge Cervical mucus Endometrial fluid Fluid from Skene’s and Bartholin’s glands Exfoliated squamous cells Normal pH: 3.5 – 4.5 during reproductive years; 6 – 8 after menopause
Vaginitis and PID Wanda Ronner, M.D.. Vaginitis Disruption in the normal vaginal ecosystem Alteration of vaginal pH A decrease in lactobacilli Growth.
Vaginitis Disruption in the normal vaginal ecosystem Alteration of vaginal pH A decrease in lactobacilli Growth of other bacteria
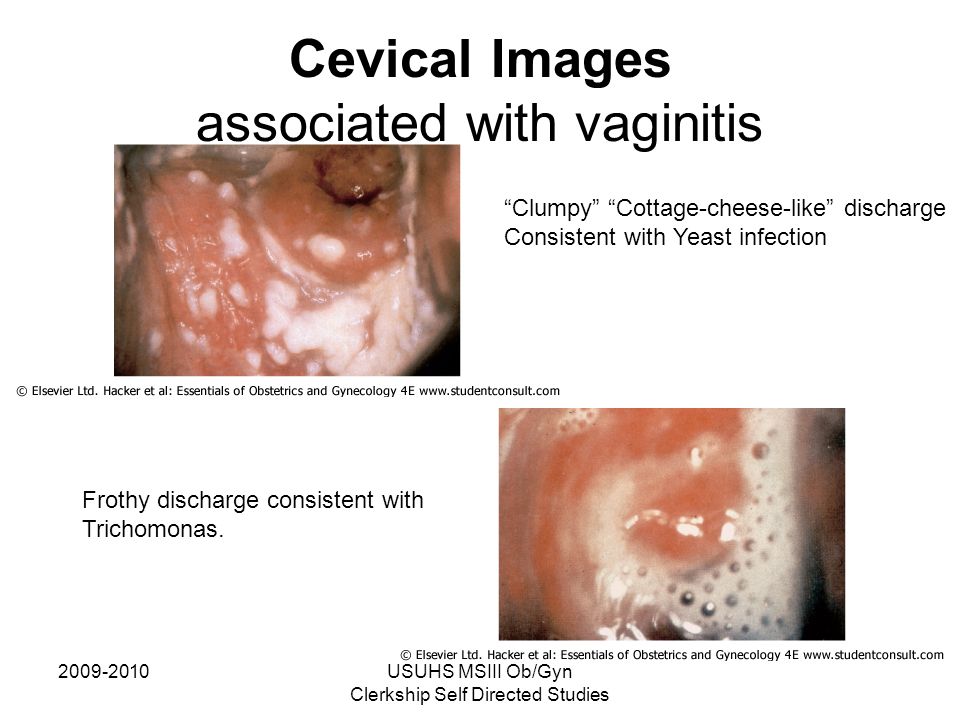
Common Causes of Vaginitis Bacterial Vaginosis: % of cases; all ages; anaerobic bacteria and Gardnerella vaginalis Trichomonas: % of cases; years; protozoan Trichomonas vaginalis Candida: 33% of cases; premenopausal women: 90% caused by Candida albicans
Trichomonas: oral metronidazole 2 grams in a single dose or 500mg bid for 7 days. Bacterial Vaginosis: oral metronidazole 500mg bid for 7 days, or intravaginal clindamycin cream or metronidazole gel..
Atrophic Vaginitis Affects 40% of postmenopausal women Caused by estrogen deficiency Symptoms: dryness, itching, burning, dyspareunia, pelvic pressure, yellowish- green malodorous discharge Findings: pH > 5, decreased superficial cells, WBCs Treatment: vaginal or oral estrogen
67 yr. old with vulvar/vaginal atrophy
vaginalis, Haemophilus, enteric Gram-negative rods, Streptococcus agalactiae..
70,000 hospitalizations/year. Most common serious infection of women age 16 – 25. One in four women have significant medical or reproductive complications..
Diagnosis of PID Cervical motion tenderness or Uterine tenderness or Adnexal tenderness Temp > 101º F Mucopurulent discharge Abundant WBCs on wet mount GC or Chlamydia
pain with ovulation) Dysmenorrhea Endometriosis UTI/Pyelonephritis Bowel disorders.
Treatment of PID Need to provide empiric, broad spectrum coverage of likely pathogens Must include treatment for GC and Chlamydia Cefotetan/Cefoxitin plus Doxycycline Clindamycin plus Gentamicin Ampicillin/Sulbactam plus Doxycycline ORAL TREATMENT: Ceftriaxone IM plus Doxycycline with or without Metronidazole
Err on the side of caution Empiric treatment of PID should be initiated in sexually active young women and other women at risk for STDs if they are experiencing pelvic or lower abdominal pain if no other cause for the symptoms can be identified.
Even mild cases may result in severe damage: infertility, ectopic pregnancy, and chronic pelvic pain..
Follow Up Improvement should be seen within 3 days on oral meds – defervescence, reduction in abdominal tenderness, uterine, adnexal and cervical motion tenderness – if not – HOSPITALIZE In no improvement after 3 days on parenteral meds consider laparoscopy

4-Female Reprooductive System, PDF, Biopsy

Vaginitis and PID Wanda Ronner, M.D.. Vaginitis Disruption in the
Infections in OB/GYN: Vaginitis, STIs - ppt video online download

Seminar VI Obstetric & Gynecology - ppt video online download
Vaginitis and PID Wanda Ronner, M.D.. Vaginitis Disruption in the
Infections in OB/GYN: Vaginitis, STIs Lisa Rahangdale, MD, MPH
USUHS MSIII Ob/Gyn Clerkship Self Directed Studies Vulvar

Vaginitis and PID: Wanda Ronner, M.D, PDF

Pelvic Inflammatory Disease (PID) - ppt video online download
CLINICAL PRACTICE GUIDELINES PELVIC INFLAMMATORY DISEASE Edelle

Vaginitis and PID: Wanda Ronner, M.D, PDF
PPT - Vaginitis PowerPoint Presentation, free download - ID:795178

Vaginitis and PID Wanda Ronner, M.D.. Vaginitis Disruption in the
Vaginitis and PID – The Basics Wanda Ronner, M.D.. - ppt download